Literatuur
Bassovitch, Oleg; Tatiana V. Serebrovskaya (2010). "Equipment and Regimes for Intermittent Hypoxia Therapy". In Lei Xi and Tatiana V. Serebrovskaya. Intermittent Hypoxia: From Molecular Mechanisms To Clinical Applications. New York: Nova Science Publishers, 2009 [265 KB]
561-72. ISBN 9781608761272 [265 KB]
Ieder jaar vindt in Cambridge, Engeland, een congres plaats over anti-aging, genaamd SENS. Vorig jaar werd IHHT genoemd als goede kandidaat om de veroudering tegen te gaan en als een praktische toepassing, die nu al gegeven kan worden. Zie ook onderstaande samenvatting afkomstig van: http://www.sens.org/node/2069
Intervall-Hypoxia-Hyperoxia-Therapy as a non-invasive tool to treat chronic diseases based on mitochondrial dysfunction
Authors:
B.-M. Löffler, E. Egorov
Institute for preventive and aesthetic medicine
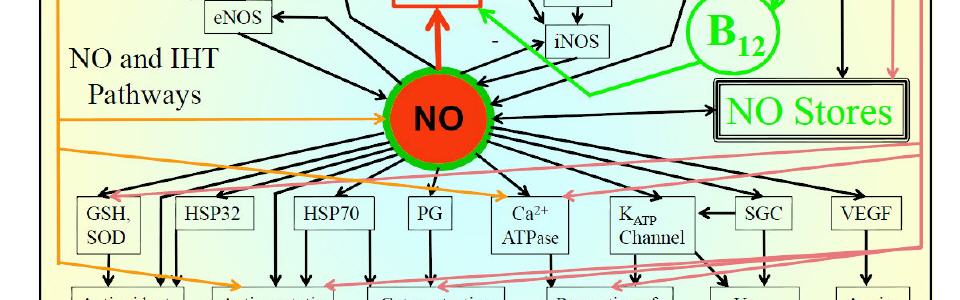
Intervall-hypoxia-therapy (IHT) is an in western medicine so far mostly unknown non-invasive therapeutic opportunity, even so that the physiological principles are at present already quit well understood down to the molecular level. With respective devices the concentration of oxygen in the breathable air is modulated between 21% (sea level) and 9% (+6500 m altitude) for defined periods. A novel element in this concept is the use of hyperoxia. Breathing air in alternating defined cycles with either decreased or increased (36% O2) O2 saturation does not only increase the O2 amplitude, but rather implements the modulation of additional physiological mechanisms, which improve cellular viability. Two principle mechanisms are modulated by hyoxia: a) The ability of the cell to store NO as Di-S-nitrosothiol-iron-complexes (DNIC) improve the physiological NO-reactivity and decreases the production of reactive nitrogene species (RNS). b) The activation of a plethora of hypoxia dependent genes, including those for erythropoetin, VEGF, VEGFR-1 and -2, Endothelin-1, iNOS, HOx-1, glycolysis enzymes, glucose transportes GLUT-1 and -3, iron metabolism, growth factors including TGF-b, PGF, PDGF-ß, HGF, apoptosis regulation factors Bcl-2, Mcl-1, Bax through the regulation of hypoxic-inducible-factor-1a (HIF-1a). On the other side hyperoxia although regulates on the gene expression level: ARE mediated phase-2 detoxifying ant antioxidant enzymes, IL8, IGFBP-2, ICAM-1, IL6, ENaC, p21, CCSP.
Intervall-Hypoxia-Hyperoxia-Therapy (IHHT) is an advancement of classical IHT which broadens the impact of controled O2 partial pressure modulation on cell metabolism and discloses new treatment opportunities. The O2 partial pressure at the cellular, even more at the mitochondrial level, is of tremendous impact for the developement / treatment of chronic multi-system ilnesses.
For example: The developement of OSA (obstructive sleep apnoe) is the consequence of an unregulated hypoxia. It leads amongst others to a therapy resistant hypertension. With heart-rate-variability controlled IHHT we could reverse the OSA in a patient with long standing OSA to normal and improve blood pressure and resting heart rate significantly. In a doulble-blind placebo controlled study with 10 IHHT treatment units of 35 minutes each we could show that the plasma Q10 level increased by 43% (p<0.01). In patients with chronic lyme borreliosis symptomatology and immunological parameters could be improved significantly. In patients with chronic diseases accompanied by high oxidative stress and imflammation, including solid cancer, colitis ulcerosa and morbus crohn, nitrosative stress and inflammation could be ameliorate significantly. Do to the regulatory impact on fundamentaly important basic cellular regulatory principles, all involved in the regulation of oxidative/nitrosative stress, chronic inflammation, and mitochondrial energy metabolism, IHHT has a very broad applicability from the treatment of serious chronic diseases to prevention and anti-aging.
Keywords:
intervall hypoxia hyperoxia therapy
mitochondrial dysfunction
Coenzyme Q10
oxidative stress
anti aging
Category:
Oral
Toepassing bij COPD
Klik hier voor de studie [211 KB]
Overzichtsartikel, IHHT goed voor hart en vaten
Zie hier voor een recent overzichtsartikel. [1.221 KB]
High Alt Med Biol. 2002 Summer;3(2):205-21.
Intermittent hypoxia research in the former soviet union and the commonwealth of independent States: history and review of the concept and selected applications.
Serebrovskaya TV.
Source
Department of Hypoxic States, Bogomoletz Institute of Physiology, Kiev, Ukraine. sereb@biph.kiev.ua
Abstract
This review aims to summarize the basic research in the field of intermittent hypoxia in the Soviet Union and the Commonwealth of Independent States (CIS) that scientists in other Western countries may not be familiar with, since Soviet scientists were essentially cut off from the global scientific community for about 60 years. In the 1930s the concept of repeated hypoxic training was developed and the following induction methods were utilized: repeated stays at high-mountain camps for several weeks, regular high altitude flights by plane, training in altitude chambers, and training by inhalation of low-oxygen-gas mixtures. To the present day, intermittent hypoxic training (IHT) has been used extensively for altitude preacclimatization; for the treatment of a variety of clinical disorders, including chronic lung diseases, bronchial asthma, hypertension, diabetes mellitus, Parkinson's disease, emotional disorders, and radiation toxicity, in prophylaxis of certain occupational diseases; and in sports. The basic mechanisms underlying the beneficial effects of IHT are mainly in three areas: regulation of respiration, free-radical production, and mitochondrial respiration. It was found that IHT induces increased ventilatory sensitivity to hypoxia, as well as other hypoxia-related physiological changes, such as increased hematopoiesis, alveolar ventilation and lung diffusion capacity, and alterations in the autonomic nervous system. Due to IHT, antioxidant defense mechanisms are stimulated, cellular membranes become more stable, Ca(2+) elimination from the cytoplasm is increased, and O(2) transport in tissues is improved. IHT induces changes within mitochondria, involving NAD-dependent metabolism, that increase the efficiency of oxygen utilization in ATP production. These effects are mediated partly by NO-dependent reactions. The marked individual variability both in animals and humans in the response to, and tolerance of, hypoxia is described. Studies from the Soviet Union and the CIS significantly contributed to the understanding of intermittent hypoxia and its possible beneficial effects and should stimulate further research in this direction in other countries.
PMID: 12162864
Ter ondersteuning van afvallen
J Physiol Biochem. 2011 Nov 3.
Usefulness of combining intermittent hypoxia and physical exercise in the treatment of obesity.
Urdampilleta A, González-Muniesa P, Portillo MP, Martínez JA.
Source
Department of Pharmacy and Food Sciences, University of Basque Country, Vitoria-Gasteiz, Spain.
Abstract
Obesity is an important public health problem worldwide and is a major risk factor for a number of chronic diseases such as type II diabetes, adverse cardiovascular events and metabolic syndrome-related features. Different treatments have been applied to tackle body fat accumulation and its associated clinical manifestations. Often, relevant weight loss is achieved during the first 6 months under different dietary treatments. From this point, a plateau is reached, and a gradual recovery of the lost weight may occur. Therefore, new research approaches are being investigated to assure weight maintenance. Pioneering investigations have reported that oxygen variations in organic systems may produce changes in body composition. Possible applications of intermittent hypoxia to promote health and in various pathophysiological states have been reported. The hypoxic stimulus in addition to diet and exercise can be an interesting approach to lose weight, by inducing higher basal noradrenalin levels and other metabolic changes whose mechanisms are still unclear. Indeed, hypoxic situations increase the diameter of arterioles, produce peripheral vasodilatation and decrease arterial blood pressure. Furthermore, hypoxic training increases the activity of glycolytic enzymes, enhancing the number of mitochondria and glucose transporter GLUT-4 levels as well as improving insulin sensitivity. Moreover, hypoxia increases blood serotonin and decreases leptin levels while appetite is suppressed. These observations allow consideration of the hypothesis that intermittent hypoxia induces fat loss and may ameliorate cardiovascular health, which might be of interest for the treatment of obesity. This new strategy may be useful and practical for clinical applications in obese patients.
PMID: 22045452
Column van Johan Bolhuis over vermoeidheid
Column gezondNU, nr. 1, 2012
Chronisch vermoeid
Moe, moe en nog eens moe
Iedereen is wel eens moe, zeker na een drukke periode of een slechte nacht. Er zijn echter mensen die dag in dag uit zo moe zijn, dat zelfs leuke dingen doen niet lukt, dat zelfs douchen bijna te veel is, een lichte inspanning als tien minuten wandelen geeft dan soms tot dagen erna meer pijn en vermoeidheid en vaak moet een afspraak of bezoek worden afgezegd omdat ze te moe zijn.
We hebben het hier over een afmattende en invaliderende moeheid. Soms staat dit op zichzelf, soms is het een onderdeel van een chronisch ziektebeeld (kanker, reuma, etc.) en soms spelen psychische factoren een rol.
Het moeilijke aan deze vermoeidheid is dat de omgeving het vaak niet kan zien, zeker als de patiënt af en toe ook een goede dag heeft en dat de patiënt weinig begrip krijgt van vrienden, kennissen en zelfs behandelaars. Artsen hebben er geen pasklare oplossing voor, al komen er steeds meer nieuwe inzichten en mogelijkheden (1).
Enkele van die nieuwe inzichten gaan over de energie productie in elke cel in ons lichaam. Simpel gezegd is iedere cel in ons lichaam een zakje met zout water met daarin een celkern, wat eiwitten, fabriekjes voor het maken van die eiwitten en energiecentrales. Die energiecentrales noemen we mitochondria en een mitochondrium is in staat om van vetten of koolhydraten pakketjes energie te maken. Deze in pakketjes opgeslagen energie worden ook wel ATP genoemd. ATP’s zijn een soort batterijen die energie leveren voor allerlei functies van een cel. Cellen gebruiken veel energie en één derde deel van deze energie wordt besteed aan het zogenaamde natrium kalium pompje in de celwand. Om te voorkomen dat onze cellen helemaal opzwellen (immers zout trekt vocht aan) pompen we steeds drie deeltjes natrium naar buiten in ruil voor twee deeltjes kalium naar binnen. Hiermee komt er meer natrium buiten de cel dan in de cel en trekt het vocht naar de plek waar meer natrium is.
Eén derde deel van onze energie gaat dus zitten in het in en uitpompen van mineralen. Als we dit efficiënter kunnen doen dan houden we misschien energie over. We hebben magnesium nodig om het pompje aan het werk te zetten en bij een magnesium tekort kun je een kalium tekort niet aanvullen. Extra magnesium geven blijkt dus mogelijk zinvol bij vermoeidheid en daar is inmiddels ook bewijs van.(2) Minder keukenzout (natrium) en meer kalium (en calcium) kan mogelijk helpen en we zien in ieder geval een betere stemming op zo’n dieet. (3)
Verder kunnen we tegenwoordig met een Engelse laboratorium onderzoek uit het bloed een ATP-profiel maken en daarin beoordelen hoe goed iemand ATP kan aanmaken en hergebruiken (4). Bij een slecht ATP-profiel kan aanvulling van stoffen (bijv. NADH of carnitine (5-7)) die nodig zijn voor de energie productie zinvol zijn. Ook blijkt uit die nieuwe testen dat mitochondria vaak minder goed werken omdat ze belast zijn met toxische stoffen. Ontgiften en een gezondere leefstijl kan daarmee zorgen voor een verbeterde energie productie. En als laatste veel belovende mogelijkheid blijkt dat je slecht functionerende mitochondria kan vervangen door nieuwe. Dit proces kan worden versneld door momenten van gereguleerd zuurstof tekort (hypoxie) vergelijkbaar met wandelen zeer hoog in de bergen. Met een medisch apparaat (IHHT) kan de hypoxie precies en veilig worden geregeld (8) en de eerste ervaringen met deze therapie laten meer energie en minder vermoeidheid zien (9). Daar krijg ik dan weer energie van.
Johan Bolhuis, arts
www.natuurarts.nl
Voetnoten: 1) PMID: 21982120 2) PMID: 1672392; 3) PMID:18466657; 4) PMID: 19436827; 5)PMID: 10071523; 6) PMID: 15377055; 7) PMID: 15039515; 8) PMID: 21033083; 9) http://www.sens.org/node/2069